Shoulder Depression: Mechanisms and Functional Differences
- Oct 27, 2025
- 5 min read

Understanding Shoulder Depression
‘Depression is accomplished through the force of gravity and the actions of the latissimus dorsi, serratus anterior, pectoralis major and minor, and the trapezius muscles.’ From https://www.ncbi.nlm.nih.gov/books/NBK531475/
To clarify, shoulder depression = shoulder girdle depression=scapular depression
We recognize that the upper limb relies on a strong and unified shoulder girdle that can move in various directions. The depression of the shoulder girdle (scapula), along with its elevation, protraction, abduction, and adduction, is understood to be a movement that plays a vital role in establishing a key link within the functional human kinetic chain.
When viewing the scapula from a traditional perspective, we see the dorsal surface in the frontal plane, as shown in the figure above. It appears to move only within this plane. A similar depiction of scapular movement is shown in the drawing I used in blog #7 (Scapular Movement: ON the ribs or With the ribs?).
When examining functional movement of the shoulder girdle, we focus on observing the scapula in the frontal plane. However, since the scapula moves in conjunction with the chest wall across multiple planes and directions, it is challenging to fully assess or understand this intricate combination of moving components.
We have a clearer comprehension of ARM movement. Flexion and extension take place in the sagittal plane, abduction and adduction happen in the frontal plane, and internal/external rotation occurs in the transverse plane. Each pair of movements is associated with a specific plane, which simplifies identifying the muscles involved in each movement.
Scapular movement is traditionally described as occurring mainly in the frontal plane, but this is not accurate. The scapula adjusts to the chest wall's contours, adapting to the arm's varying demands and positions. It moves in three dimensions, as well as superior/inferiorly.
Clinical evaluation of scapular movement should address its functional motion. At present, assessment of scapular adduction or abduction, for example, is never included in a shoulder exam because these movements, as described in the frontal plane, do not exist. We cannot clinically isolate the muscles believed to be responsible for a movement that never occurs.
Abduction and adduction are appropriate terms for describing movement at a hip or glenohumeral joint. The shoulder girdle, however, has a much different, much more complex path of movement.
From a clinical perspective, the complex motion of the shoulder girdle is essential for the function of the upper extremity. It provides stability and mobility to the upper quadrant by continually adjusting its position on the chest wall.
The gravitational force and the need for continuous functionality require almost constant adjustment of the muscles that support the shoulder girdle. We have pinpointed the muscle groups responsible for each movement of the scapula. For example, the latissimus dorsi, serratus anterior, pectoralis major and minor, and the trapezius muscles all play a role in scapular depression. However, how this muscle activity might change with variations in the scapula's position on the chest wall is still uncertain.
Elevation and depression of the shoulder girdle seem simple, as the scapula appears to merely move up or down. However, similar to abduction/adduction, the functional elevation and depression of the shoulder girdle need to follow the three-dimensional contours of the chest wall.
"Shoulders Back" vs. "Shoulders Forward"
Shoulder girdle depression can occur with the arm in virtually any functional position.
When the arm is hanging at the side of the body, the shoulder girdle sits in a 'neutral' position.
The generally accepted average 'neutral' resting position for the scapula is when it lies on the chest wall at 33 degrees of internal rotation and 8 degrees of anterior tilt. Nevertheless, the shoulder girdle's resting position varies for each person and can change depending on factors such as the time of day, age, sex, health condition, and mental state.
See the drawing below.

Posture, or in this situation...resting position of the shoulder girdle, is fluid. As a result, all three of these drawings might represent someone's 'neutral' or resting posture.
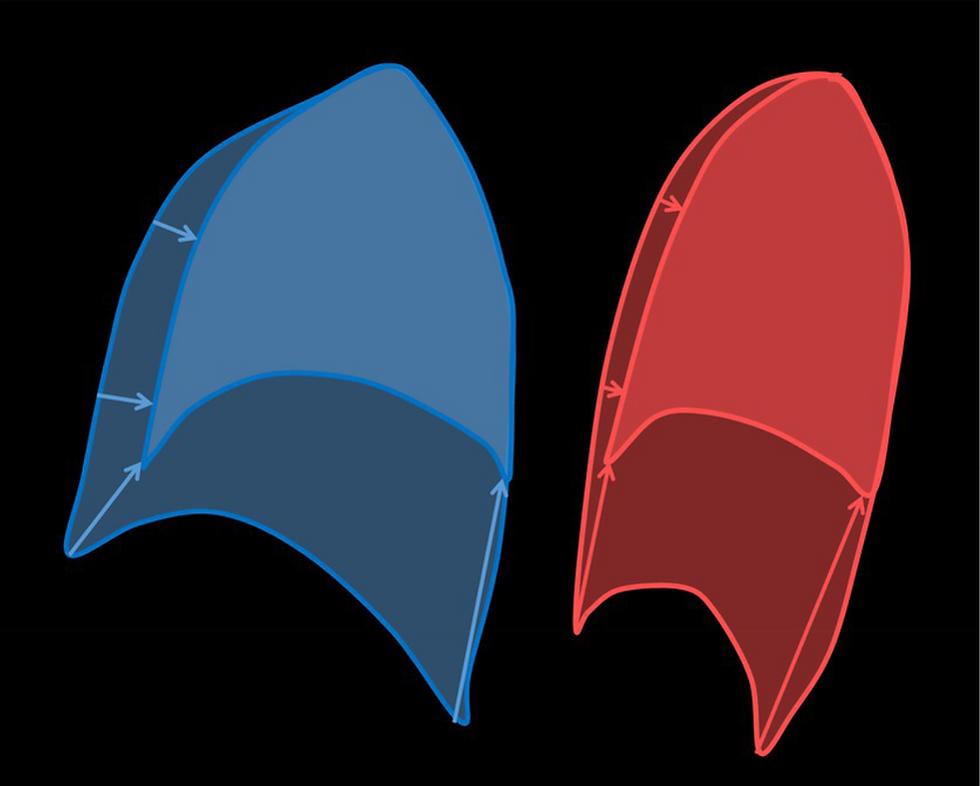
At the bottom of the illustration above, there are three corresponding conceptual figures. These unusual figures resemble tadpoles, but they were drawn to visually depict the sagittal view of the shoulder girdle's range of movement. Their peculiar shape illustrates the extent of movement the shoulder girdle might achieve. The dot at the center of each figure indicates the position of the acromion as the shoulder girdle moves in front of, over, and behind the apex of the lung. The curved line at the bottom represents the curved surface of the lung's apex.
As the clavicle and acromion swing forward and backward over the apex of the lung, they either draw the shoulder girdle "up and over" or "back and down".
An inferior glide of the shoulder girdle can occur when the shoulder girdle sits at the highest point of the lung in a 'neutral' position, but there is very little range of motion here. Downward movement of the shoulder girdle must, for the most part, occur either in front of or behind the mid-point of the apex of the lung.
Most of our daily arm movements take place in front of the body and below shoulder level. With the clavicle and acromion drawn forward, the shoulder girdle can elevate and depress (refer to #1,2 in figure 2.26 below). When additional downward force is necessary, the latissimus dorsi, pectoralis major, and pectoralis minor are ideally positioned to provide this extra force. The shoulder girdle moves forward and downward, as shown in the sagittal illustration. Medial scapular rotation and anterior scapular tilt also occur, but a different viewpoint is needed to fully understand this three-dimensional positional change. Research on three-dimensional scapular movement is well-documented, with significant early studies by McClure et al. 2001, and Ludewig 1996. A straightforward summary can be found in my book, "Scapulothoracic Assessment in Three Simple Steps," on page 21.
Reaching backwards into extension, from the neutral starting position (not shown), the shoulder girdle moves further into the anterior/inferior + medial rotation and anterior tilt position.
As the arm is elevated toward 90 degrees and above, the shoulder girdle travels backward (2), and back/down (3,4). When observed three-dimensionally, there is also increased scapular external rotation and increased scapular posterior tilt as the arm is elevated.
This drawing represents only one of three planes of movement and is not drawn to scale, but it does illustrate anterior, posterior and inferior shoulder girdle translation that occurs as the arm travels overhead.

Most functional shoulder girdle depression, therefore, happens during normal shoulder function. Not when we actively try to "depress" the shoulder girdle, but when it moves in front of or behind the sagittal midline as it accompanies active movement of the arm.
Anteriorly, shoulder girdle depression is accompanied by scapular internal rotation and anterior tilt. Depression forces, other than gravity, are provided primarily by the latissimus dorsi and the pectoralis muscles.
Posteriorly, shoulder girdle depression is accompanied by scapular external rotation and posterior tilt. The ONLY muscle that is capable of providing shoulder girdle depression, in combination with posterior tilt and external rotation of the scapula, is the SERRATUS ANTERIOR.
The trapezius is engaged during the elevation and depression of the scapula, but its main function is to facilitate posterior scapular rotation. Refer to Johnson et al. 1994 or "Scapulothoracic Assessment in Three Simple Steps" by J. Delorme, 2021, pages 22/23.
Now, let's look at our opening statement again:
‘Depression is accomplished through the force of gravity and the actions of the latissimus dorsi, serratus anterior, pectoralis major and minor, and the trapezius muscles.’
This statement is still true, but with a better understanding of how the shoulder girdle moves during function, it is possible to isolate a shoulder girdle position where the serratus anterior works alone to secure the necessary scapular depression on the chest wall.
Although the serratus anterior performs several functions that are frequently overlooked, it can now be recognized as the primary muscle responsible for scapular depression when the scapula is rotated externally and tilted backward.
This insight has clinical implications...


Comments