Scapular Movement: ON the ribs or WITH the ribs?
- Jun 5, 2023
- 7 min read

In Blog #5, we asked these two questions:
1. How does the scapula perform its important job, as a ‘coupler’ …serving as a link, that transfers energy…
2. How can we measure or identify whether this ‘coupler’ is working as it should?
Today, we answer these questions, but to begin, we ask a third question:
Does the scapula slide around on the surface of the thorax like a curling rock on a sheet of ice, or does the scapula ‘couple’ with the ribs as the arm moves up and overhead?
Blog #6 provided detailed morphology of the serratus anterior (SA) muscle. This serrated, balanced, three-dimensional muscle has intimate contact with the front of the scapula. It is attached to the tops of ribs #1-8 and sometimes 9 and to the upper and lower surfaces of
rib # 2. From most of the medial scapular border, SA fascicles travel forward, either in a horizontal plane (middle fibres) or in a downward direction (upper and lower fibres) toward their rib attachments. Remember, these observations and measurements are from a cadaver, with the arms resting at the side of the body.
Photo from Webb et al. 2016.

Consider the “Setting Phase” …
1. The first rib is short, strong, and thick, with a solid connection to the sternum (axial skeleton). When the upper division of SA contracts, fascicles from the first and second ribs (via R2s) will lift the first rib and draw it slightly posterior. This will create a solid connection between the scapula and the upper thorax. This strong connection can provide stability for the upper thorax and an axis for scapular rotation.
2. The middle division, with a shared myofascial connection at rib #2, will be drawn upwards and medially, toward the first rib. This upward force on rib two, combined with the horizontal/medial forces from R2i and R3 will create some compression at the rib joints, and will increase myofascial tension within the thin but expansive middle division fascicles. This increased tension ‘connects’ the upper and lower parts of this muscle.
3. The powerful lower division (T4-8 or 9) can now engage. Remember, the arm is still resting at or near the side of the body. With the upper 2/3 of this muscle secured, the lower fibres contract and draw the scapula downward* and outward – slightly. Contraction of the lower division fascicles will complete the process. The entire muscle is now ‘engaged’ or attached to the ribs and is ready to move “with” the chest wall. This is the “Setting Phase”.
…A simplified description to be sure. Other scapulothoracic muscles are needed to ‘offset’ the activity of SA, for example, the rhomboids and the levator scapula will be needed to stabilize and support the medial scapular border. Digressing into this discussion, however, will only make this blog more complicated. With 17 muscles acting on one coupler, and others acting indirectly through the arm, understanding arm attachment is a process, so it is important to study one part of it at a time.
* If results from s 2006 paper by Smith et al. can be recognized as reliable, the lower fibres of SA do contract relatively strongly when the participant is attempting shoulder girdle depression with the arm resting at the side of the body.
My personal experience with this – be sure to instruct the participant: “Do not pull down with the arm”. The latissimus dorsi will attempt to assist with shoulder girdle depression unless you are careful with instructions.
SA (acting like a ‘cinch’ holding a saddle on a horse) has ‘coupled’ the ribs with the scapula, and now they are ready to move together.
Inman et al. observed the ‘setting’ phase occurred during the first 60 degrees of movement when the arm was lifted in front of the body (sagittal plane), yet only 30 degrees of arm elevation was required when it was lifted at the side of the body (frontal plane). This difference is easily explained, and it also sheds some light on why scapular movement during the setting phase varies so much from one person to the next – everyone has a unique resting posture, therefore a different starting position.
When establishing a ‘cinch’ between the scapula and the chest wall, the starting position of the scapula is important. If the arm is in front of the body when the arm starts to elevate, the scapula will be positioned a little further from the midline because it has been drawn forward and around by the arm. The SA, when engaged, will first restore the scapular resting position so it can create the best possible contact with the chest wall and the shortest, most efficient axis of rotation for the scapula.
The critical thinkers who are reading this blog are already asking…
How do you know that the ribs move when the arms move, and if they do, how do they move?
A research project by Tachihara and Hamada, 2019
evaluated movements of the ribs and the thoracic spine as both arms were lifted overhead.


Tachihara and Hamada 2019
Their results indicated that the thoracic spine and all 12 ribs move as the arms are lifted.
The most movement (9.4 mm) occurs at the fifth rib, and the farther from the fifth rib, the smaller the movement of the rib. See the graph below:


Tachihara and Hamada 2019
The results also indicated that aging and gender influenced rib movement.
Does the SA, on its own, provide rib movement and improve chest wall stability as the arms are being raised overhead?
We don’t know. There are many muscles and other connecting tissues that may contribute to rib movement and rib stability.
I suggest that the scapula and the serratus anterior, when “cinched” together, may provide some increased stability, to BOTH the chest wall and the arm attachment.
A stable scapula/chest wall connection needs to begin when gravity begins, when the torso is upright and the dependent arms are resting at the sides of the body (this is a separate discussion – details in my BOOK ONE).
If more stability is required, raising the arm, for example, additional muscles will need to participate. As they do, the stability and movement contribution from the chest wall will need to be adjusted. The SA, contracting with increasing intensity (and in concert with other scapulothoracic/scapulohumeral mm – primarily trapezius), will create additional superior/medial force through its distal rib attachments (ribs #1-8 or 9). This superior/medial force will result in rib movement, as compression at the rib joints and tension between the ribs gradually increases.
Changing the position of the ribs will create stability and strength within the thorax… the ‘core’ of the kinetic chain’. Think about winding up an old-fashioned clock or adjusting a thermostat. The scapula rotates, and as it does so, it behaves like a ‘rheostat’, creating the correct balance of compression and tension within the thorax. The thorax provides stability and strength to the arm, of course, but it also provides the stability that is necessary for the transfer of forces throughout the body. The glenohumeral joint… yes, it is impacted, because it is part of the human kinetic chain. But, considering the magnitude of the entire kinetic chain, participation of the glenohumeral joint within it should be recognized as one part of a very large puzzle, or perhaps, the tip of an iceberg.
Upward scapular rotation…with and without SA


Photo (L) - Left SAP. Illustration (R) recopied from Kendall, 1993 - (R) SAP
In both examples, above, the ‘normal’ arm elevates fully and is engaged with the thorax. The SAP side demonstrates upward scapular rotation, but the scapula is not engaged with the thorax. It has drifted upwards…brought there by scapulohumeral muscles and trapezius.
Upward scapular rotation does occur without serratus anterior, but it does so without the support of the thorax.
If the scapula follows the convex shape of the chest wall as the arm is lifted, the shape of the chest wall will dictate posterior tilt. The scapula must maintain its ‘cinch’ connection with the ribs if posterior scapular tilt is to accompany arm elevation.
Behaving as a supported unit, this connection can again be compared with our horse and rider –
If the ‘cinch’ is tight enough, the saddle does its job correctly. If it is loose, the rider will move around in an unpredictable fashion. In other words, the rider will present with some ‘dyskinesis.’
With a snug connection, the saddle and rider will move TOGETHER. The rider will move with the horse. The scapula, when correctly 'cinched', will move with the thorax. The movement will be very predictable.
When the scapula is not “cinched” or engaged onto the chest wall, it can move with some freedom. The extent and direction of “disengaged” scapular movement will depend, of course, on body type, arm and body position, and the strength and flexibility of other scapulohumeral, scapulothoracic and axiohumeral muscles.
For example: Increased pull from the latissimus dorsi, combined with insufficient support from the scapulothoracic mm, will allow downward scapular tilt. In a younger, healthy individual, the scapular dyskinesis, shown here, will likely not present as a problem. If multiple risk factors were at play, however, symptoms would, in time, start to present themselves.

So, to answer our question from the beginning of this blog:
Does the scapula slide around on the surface of the thorax like a curling rock on a sheet of ice, or does the scapula ‘couple’ with the ribs as the arm moves up and overhead?
Both
When the scapula IS cinched to the chest wall, then its movement will mirror that of the ribs. Changes in scapular posterior tilt and upward rotation are dependent upon rib movement, and rib movement varies significantly with sex and age.
When the scapula IS NOT cinched to the chest wall, muscles alone control scapular position and movement, and the scapula moves freely and less predictably.
Looking only at the scapula can provide a starting place for the assessment of dysfunction in this region, but to understand the source of a scapulothoracic problem, it may be necessary to look somewhere else.
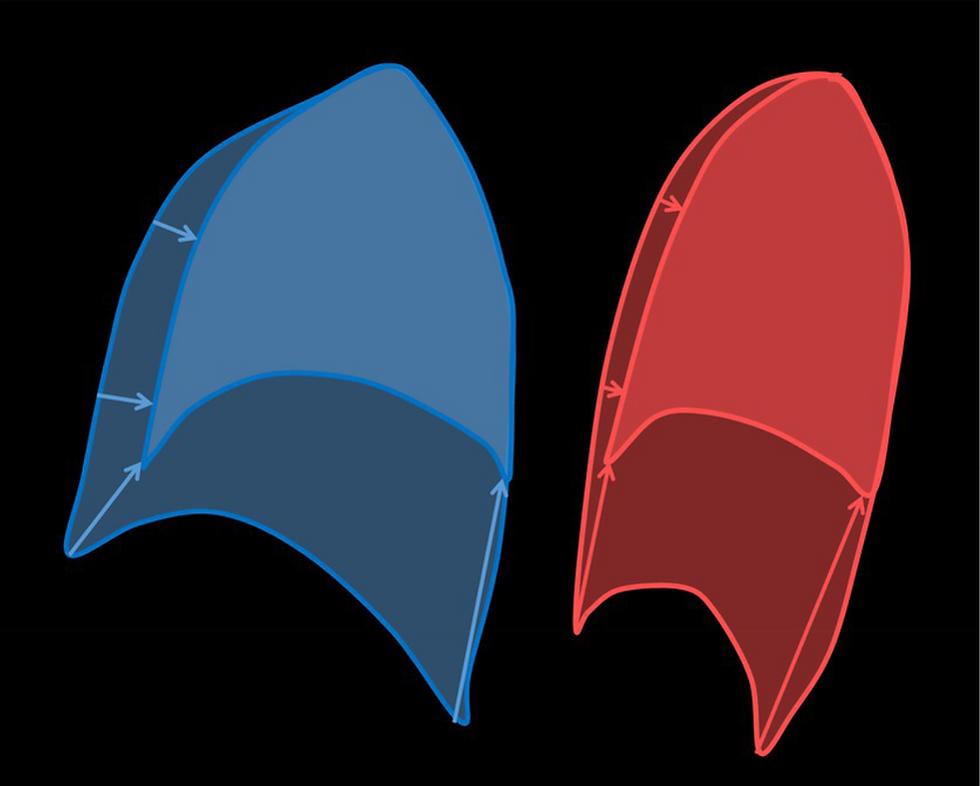
In this short video, we are looking at rib movement and rib stability. The right side is normal, and the left side has a palsy of the SA muscle. The differences are hard to miss.
Thanks for reading and watching.
I am looking forward to feedback from readers. I would like future blogs to reflect what readers are interested in discussing…
Coming next, I thought that a look at epidemiology might be interesting. We can investigate who, among the general population, struggles the most with ‘shoulder’ pain…


Comments